
Congenital Adrenal Hyperplasia
An overview
Growing up with a medical condition such as Congenital Adrenal Hyperplasia (CAH) can be very difficult. The problems of having CAH can be considerably reduced if the right type of information is made available and discussed sensitively. As young adults the issues of sexuality and fertility need early discussion so that adult life can be approached with confidence. These issues can be difficult for some parents, children and doctors.
As with any medical condition there are wide variations as to how each person is affected by CAH and not all that is in this leaflet will be relevant to everyone. For instance, CAH has different effects on women compared with men. This leaflet describes how some adults see the condition of CAH affecting their lives. Addressing these feelings enables them to find ways to deal with them. Further support may be found through the family, friends, a support group, a counsellor or a doctor. A specialist with a particular interest in the problems associated with CAH is needed at times.
What is Congenital Adrenal Hyperplasia?
The adrenal gland sits above each kidney – one on each side of the body. It is made up of a medulla (middle) which makes adrenaline – this part works perfectly normally in CAH. The outer part of the adrenal gland is the adrenal cortex which makes three main hormones called steroids. These steroids are secreted into the blood stream and are necessary for normal health. It is the adrenal cortex and its hormones which are involved in CAH.
The 3 main steroids involved in CAH are:
- Cortisol controls how the body copes with stress, emotional and physical, such as infection or injury. It also helps to control blood sugar levels, raising these levels if they become too low particularly in children.
- Aldosterone helps to regulate the salt levels in the body. Aldosterone causes the kidneys to conserve salt if there is too little salt in the diet, or if a lot of salt is lost due to excessive sweating. Conversely, if a lot of salt is eaten the adrenal cortex reduces the amount of aldosterone secreted, allowing the excess salt to be passed in the urine.
- Androgens are a group of male hormones, one of which is testosterone. For the rest of this booklet the term testosterone will be used to refer to the androgen group. Testosterone is produced by the adrenal cortex in both males and females and they control the formation of pubic hair at the onset of puberty. Testosterone is also produced by the testis and in small amounts by the ovary.
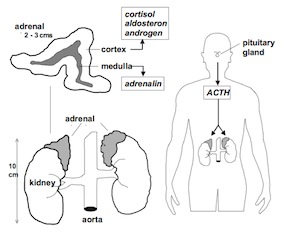
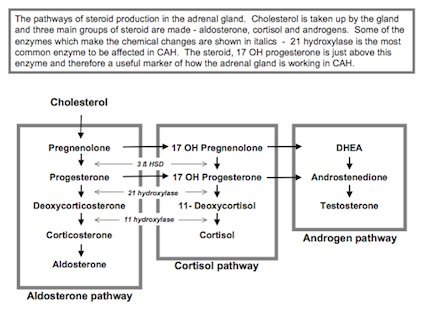
There are five main enzymes in the adrenal gland which convert cholesterol into the important steroid cortisol. If any of these enzymes are missing or defective then not enough cortisol is made for the needs of the body. The body, recognising the low levels of cortisol, will try to stimulate the adrenal cortex to make more by ‘pushing’ the gland harder by a stimulating hormone called ACTH made in the pituitary gland. The constant unsuccessful stimulation causes the cortex to increase in thickness and become ‘hyperplastic’.
In the most common form of CAH there is a deficiency of an enzyme called 21 hydroxylase. In this form of CAH the production of cortisol and aldosterone is low while testosterone, the male hormone, is produced normally. As the body pushes the adrenal gland harder trying to correct the low cortisol level more and more testosterone is made. In boys, this excess of testosterone causes early sexual development. In females, the excess in testosterone can cause abnormal genital development before birth while in adults it causes irregular periods, unwanted hair growth and acne. Only by correcting the levels of cortisol with substitute therapy does the body recognise normal levels and stop producing excessive amounts of testosterone and the circulating levels become normal.
The hormone disturbances caused by CAH
- Lack of cortisol
- Lack of aldosterone
- Excessive androgens
Different types of CAH
There are many different grades of severity of CAH depending on the degree of impairment of production of cortisol and aldosterone. In the most severe type of CAH aldosterone is completely lacking and loss of salt from the body is the most prominent problem – salt losing CAH accounts for 80% of children with CAH. The loss of salt in the urine is uncontrolled and can cause acute dehydration, very low blood pressure and vomiting. The levels of salt (sodium and chloride) and sugar (glucose) fall in the blood, and the potassium level rises. This is an ‘Adrenal Crisis’ needing very urgent treatment as a potentially life threatening condition. In the 20% of children with less severe CAH, non salt-losing CAH, the salt balance is normal. In stressful situations, however, some people with non-salt losing CAH may become salt losers and need extra treatment. Girls born with non salt-losing CAH are usually healthy, but are often born with an enlarged clitoris and the labia may be partially fused because of the excess of testosterone. In boys, non salt-losing CAH produces no detectable signs at birth and the diagnosis is made when the penis enlarges at a very early age along with early pubic hair and rapid growth in height the result of high levels of testosterone. These changes may not occur until 4 or 5 years old.
The mildest form of CAH – late onset CAH - affects women at any age. Symptoms of unwanted hair growth or irregular periods can start at any time after puberty. Often treatment with steroids is not necessary in women with late onset CAH. Instead, giving oestrogen as in the oral contraceptive can regulate testosterone from the ovary. In fact, the treatment of late onset CAH is usually the same as for the polycystic ovary syndrome because the two conditions are so similar. In men, late onset CAH usually goes unrecognised although it may cause the sperm count to be low.
All of the types of CAH above are deficiencies of the enzyme 21 hydroxylase which account for over 90% of people with CAH. The next most common deficiency is of the enzyme 11-beta hydroxylase. Treatment of this type of CAH is more complicated because high blood pressure can be severe if treatment is inadequate. The balance of treatment in 11-beta hydroxylase deficiency is very difficult and an experienced specialist is essential. Deficiencies of other enzymes are exceedingly rare and beyond the scope of this pamphlet. A specialist will be able to offer more information on the rarer forms of CAH. Adrenogenital syndrome is an older name for CAH which is still used occasionally.
Treatment of CAH
People with CAH have a normal life expectancy and for most people there is very little interference in every day life if the condition is well managed. Adults with CAH require life long follow up in specialist hospital clinics in order to maintain the correct level of medical care and to provide early advice on fertility when needed.
It is advisable to have regular medical checks even if everything is well controlled. For women, checks should be made 2 - 3 times per year. For men, once per year is usually sufficient. The main aim of treatment is to maintain normal cortisol levels and control of salt loss, in those who are salt losers. In women, good management of CAH brings about control of testosterone levels, regular periods and improved fertility. In men, good management can reduce an aggressive behaviour and control excessive libido. Also, the sperm count can fall if CAH is not well treated and an increase in the dose of steroid treatment for some months can restore fertility in men.
Replacement of cortisol
The object of cortisol treatment in CAH is to replace inadequate production of cortisol by the adrenal glands allowing the body to recognise normal levels of cortisol in the body, which reduces the need for the adrenal gland to produce excessive amounts of testosterone.
How do doctors work out how much cortisol to take?
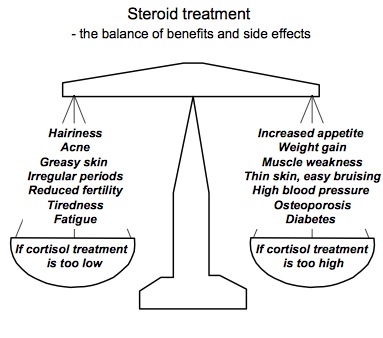
If the cortisol dosage is too low the adrenal gland will try and make more, but only succeed in making more testosterone. The effect of these excess androgens is growth of body hair in women and infertility in both sexes. In severe forms of CAH, too little cortisol treatment may make the body unable to cope with stress and infection, so that major surgery or an illness like ‘flu’ can be life threatening. If the dose of cortisol treatment is too low, a blood test will establish this by showing high levels of several adrenal hormones of which the most commonly measured are:
- 17 Hydroxyprogesterone
- Androstenedione
- Testosterone
Water retention (sometimes associated with taking Hydrocortisone and Cortisone acetate)
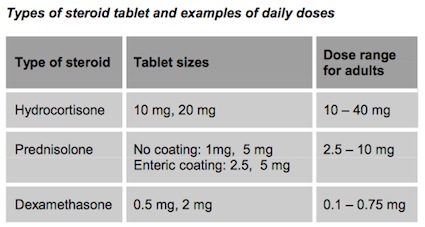
There are four types of cortisol replacement treatment: Hydrocortisone, Cortisone acetete (now rarely available in the UK), Prednisolone and Dexamethasone. They vary in their dose and duration of action. Hydrocortisone is another name for cortisol. Prednisolone is 5 times more potent, and dexamethasone is 40 times more potent than cortisol. Both prednisolone and dexamethasone are comparatively long acting, where as cortisone acetate and hydrocortisone are shorter acting, and need to be taken 2 to 3 times a day. The dose in each dexamethasone tablet is not convenient for fine-tuning of treatment leading to a danger of taking too high a dose. Dexamethasone is established for use in pregnancy for women who are at risk of having a child with CAH. Hydrocortisone is also used as an injection at times of adrenal crisis or when vomiting prevents the tablets from being taken.
The exact dose needed each day for each individual will differ, due to the variation in body size, different rates of absorption in the bowel. It is important to assess the individual response, taking into account timing of the day that medication is taken. It is important to be clear how many tablets are missed so that the correct balance of dosage can be achieved. Many people find it difficult to take tablets regularly and this can lead to conflict with doctors.
At times of stress such as during illness or physical or emotional shock, the dose of cortisol replacement treatment should be increased in a controlled way. The exact regime should be agreed in prior discussion with you doctor. For example, a double or treble dose is usually advised at times of stress. The body increases cortisol in situations of high mental stress and it may therefore be necessary to give an increased dose even if only for one day for exams,a driving test, or a sudden bereavement for example. If an illness causes prolonged vomiting which prevents tablets from being taken, then an injection of hydrocortisone 100 mg should be given into the muscle and a doctor should be called. The technique of injection can be learnt by members of the family with instruction from the practice nurse.
Unless there has been substantial over dosing of fludrocortisone, blood pressure should not present a problem taking into account the wide variation in general blood pressure levels.
Replacement of aldosterone
All individuals with salt losing CAH need to replace the lack of aldosterone. Only one form of treatment is used here. Fludrocortisone is given in a dose of 50 – 300 micrograms. Too little fludrocortisone can cause low blood pressure and dizziness. Too much fludrocortisone can cause high blood pressure and headaches. The correct level of fludrocortisone is determined by measuring blood pressure, potassium and the salt sensitive hormone renin in the blood every few years.
Adrenal crisis
If there is a severe shortage of cortisol then an individual’s life can be in danger with an adrenal crisis. This event is very rare and will never happen to most people with CAH who take treatment regularly, make appropriate increases in dose when ill and seek help early if unexpectedly unwell or vomiting. The symptoms are faintness, nausea, vomiting and abdominal pain. An adrenal crisis can be triggered by a stressful illness such as severe flu or gastro- enteritis. An injection of hydrocortisone should be given immediately. Admission to hospital may be needed so that fluids can be given into a vein – a ‘saline drip’. If in doubt – always give an injection of hydrocortisone and go to the nearest accident and emergency department.
Why not take the adrenal glands out?
There is an operation to remove the adrenal glands called adrenalectomy. People who have no adrenal glands, a condition called Addison’s disease, require the same medication as those with CAH, so the question sometimes arises that if treatment is difficult for any reason, why not remove the adrenal gland? Adrenalectomy is not a minor operation and the long-term safety of this option has not been established. For some women in whom all fertility treatments have failed, then adrenalectomy might be the only answer.
Issues for adults with CAH – men and women
The problem of being over weight
Many people with CAH, women in particular, have a battle to avoid gaining weight. Mostly, weight gain in CAH is a side effect of treatment with hydrocortisone, prednisolone or dexamethasone and to a lesser extent, the oral contraceptive pill if used. Short stature and depression can also make weight gain more likely. Careful monitoring of weight is important as prevention of weight gain is better than a harsh weight reducing diet. Careful adjustment of treatment and attention to diet and exercise should enable most people with CAH to avoid obesity. A normal healthy diet which is low in sugar and fat and high in fibre is best. A sugar craving can be hormone driven although the effect of various treatments is unpredictable. Regular sustained exercise of an hour several times per week may be required to keep fitness levels up and weight down.
Will my baby get CAH?
It is very rare for a parent with CAH to pass the condition on to a child – less than 1 in 100 chance. CAH is autosomal recessive condition meaning that one copy of a defective gene must be inherited from each parent to make an individual who is homozygous for CAH. A parent with CAH has two defective genes but their partner is likely to have two normal copies that will make up for the defect. That is, children of a parent with CAH will have one defective gene and one normal gene. They will be heterozygous for CAH – a situation which has no effect on health. It is current practice to test the partners of people with CAH by measuring 17-hydroxyprogesterone in the blood rather than to have a genetic test. The chances of anyone with no symptoms or family history of CAH carrying a defective gene for 21-hydroxylase is between 1:50 and 1:100. The issue of genetic testing should be discussed with your specialist well before you are planning a pregnancy because some tests are useful if performed ahead of time. The advice on this topic is likely to change with time so specialist advice should be sought as part of pre-pregnancy counselling.
Who should have genetic testing for CAH?
A change in the genetic code of the gene that is responsible for making the enzyme 21-hydroxylase is the most common cause of CAH. There are only a few centres in the United Kingdom and elsewhere, where this genetic code can be 'deciphered' and the defect can be precisely defined. Knowledge of this genetic defect in CAH has practically no effect on treatment and so the tests are not performed routinely. The only time that a genetic test is useful is to diagnose CAH before birth so that the foetus can receive early treatment by giving dexamethasone to the mother. In this way, a masculinisation of the external genitalia of female foetus with CAH can hopefully be prevented. In practice, genetic testing and antenatal treatment is only useful for families with one child already affected by CAH when the chances of having another child with CAH is one in four.
Sports
There is no restriction in any type of exercise for individuals with CAH. Indeed exercise promotes good health and helps with both weight control and the prevention of osteoporosis. With strenuous exercise an extra dose of steroid treatment is advisable especially in the early stages of training.
For those who wish to enter competition sports, the International Olympic Committee recommends declaring CAH and that steroids are being taken for medical reasons. The IOC is unable to comment on whether hormone replacement steroids needed by those with CAH would affect the status as a competitor. They are not willing to be precise on drug testing procedures which would probably include testosterone and related compounds. They consider this an important issue, and with further investigations in the future, would try to establish the effect of medication necessary in CAH on the screening tests.
The Amateur Swimming Association can see no reason to exclude any one with CAH from competitive swimming, but recommended that the ASA should be informed of the competitor’s condition prior to the event.
Travel
There should be no restriction for travel or recreation for individuals with CAH. If activity is likely to be stressful or if the destination does not have easy access to modern medical facilities, then is it wise to travel with hydrocortisone for injection. Vials of hydrocortisone for injection with syringes and needles should be taken and a dose of 100 mg given into the buttock in cases of trauma or severe vomiting. This action will make the situation safe until a doctor can be called. Supplies of hydrocortisone should be divided between hand luggage and other baggage to that in the case of one supply being lost or stolen there is always a back-up. A letter from a consultant can be useful so that contact can be made if illness occurs and to document the need for syringes and needles. Long-haul flights can be stressful and a double dose of steroids is advised.
Employment
In general there should be no restriction for employment for individuals with CAH. Commercial pilots, police, fire brigade and the armed forces are special cases where almost any condition requiring regular medical treatment can prevent employment.
Social concerns
As has already been said, those who have been able to have an open and informed relationship with their parents and doctors find the hurdles of CAH easier to overcome.
Adolescence is often a difficult time. If, added to this you have a condition which requires you to take regular medication, you may “different” and vulnerable making you unsure about relationships. Adolescent girls with CAH may need a lot of support. In all adults there are times when depression occasionally can lead to feelings of suicide. Some women with CAH feel that extreme mood swings are often caused by hormone imbalances and these concerns need careful, sensitive discussion with a specialist. For young adults and women, counselling can be of great help in establishing self- esteem and confidence and in developing strategies to cope with difficult situations that may be experienced with relationships. With a counsellor, it may be helpful to discuss and understand more about the condition. For many it will be the first time that they can talk openly about the issues of sexuality, how they perceive their bodies and female needs and how the individual sees the effect of CAH on their adult life
How and when to tell a partner about CAH can be a difficult problem. If you have confidence about your self it is much easier to put the condition into perspective for the person you are telling. Just because they now know you have CAH, this does not mean you have changed from the person they knew or loved before. This is not to be dismissive of the very real feelings a lot of women have about the fear of rejection from a potential partner. Feelings of being and looking different can put women off even trying to establish a relationship and may also cause overwhelming despair and depression. Some women find that talking to a counsellor who is not emotionally involved, can be of great help in generating confidence in herself.
The importance of adequate professional counselling has not really been addressed in many hospitals. Ideally it should be given by counsellors who understand CAH and the issues that arise from it. Always ask your doctor about counselling if you feel that it may be helpful. Some women find talking to others with CAH more helpful, as they feel they may well have experienced the same difficulties, but found ways to overcome them.
Frequently asked questions about CAH
What should I do if I miss a steroid tablet?
If it is only a few hours since the dose was due, then take the treatment when you first think of it. If the next dose is nearly due then don't take a double dose - just leave the missing dose out.
What effect does drinking alcohol have in my treatment?
Moderate drinking of alcohol has no effect on CAH or its treatment. Large amounts of alcohol can affect how the liver breaks down steroids making treatment less effective. However, if you are drinking excessive amounts of alcohol then you have more to worry about than your CAH!
Can people with CAH be extra aggressive?
An excess of testosterone when CAH is under treated can lead to aggression. However, many things in life can contribute to aggressive behaviour including having a condition for which there is no cure and facing frustrations with relationships or with fertility problems. The advice of both a hormone specialist and a psychologist might be helpful here.
What are the long-term effects of steroid treatment?
In the modern era when the doses of steroids tend to be lower than in the past, no long term problems with steroid use are anticipated. If there have been times when high doses of steroids have been used then osteoporosis is about the only long term hidden problem. A measurement of bone mineral density can be made to test for this risk.
I seem to get a lot of infections - can this be part of CAH or its treatment?
Steroids - not CAH itself - can lower the effectiveness of the immune system. For instance, people who use high dose steroid treatment after an organ transplant are more prone to various infections. The standard doses of steroid treatment used in CAH should not have this effect but occasionally it seems that some people are particularly sensitive to one of the effects of steroids such as immunity. If frequent infections are a problem then specialist advice should be sought but doctors often have no easy answer to this problem.
I don't get on with my doctor, what should I do?
Your relationship with your doctor is personal thing - some work and some don't. It is worth while trying to find a doctor whom you find sensitive and understanding as you may need them for a long time. Try talking to friends or support group members about who they find helpful. Don't be afraid to try a few out or to get a second opinion. Also remember that there may be times when you need a technical expert who may not be the worlds best communicator.